In the remote, rugged hills of Baitadi district, where paved roads are a luxury and ambulance sirens are a distant urban sound, accessing emergency healthcare has always been a race against time and terrain. For the residents of Ward No. 3 of Shivanath Rural Municipality, this critical gap is now being bridged by an innovative community-driven agreement between a local health post and a farmers’ group—a model of local partnership that is saving lives one liter of fuel at a time.
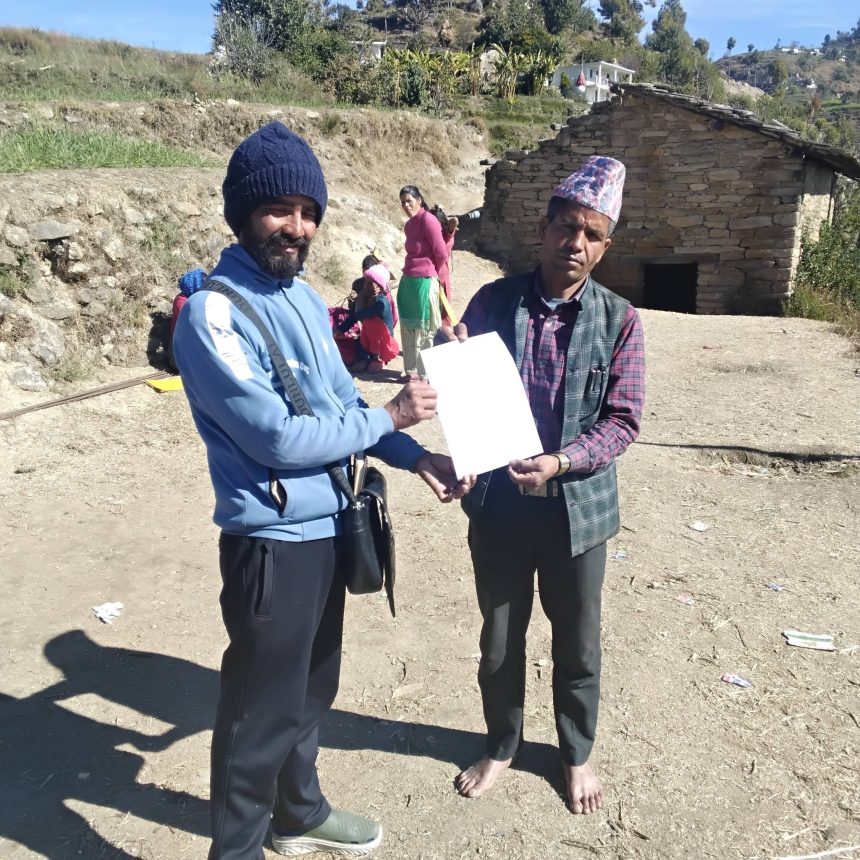
The “Shripur Health Service Center, Bachha, Baitadi” (First Party) and the “Jay Nagarjun Multi-Purpose Farmers Group, Shivanath-03, Pudil, Baitadi” (Second Party) have entered into a formal 10-point Memorandum of Understanding (MoU), creating a structured volunteer patient transport system. This agreement, signed on the 15th of Magh, 2082 BS, is not just a document but a lifeline for communities previously hours away from formal medical help during emergencies.
The Genesis of a Grassroots Solution in Baitadi

The core challenge was stark: during medical emergencies—be it childbirth complications, injuries, or acute illnesses—patients had to be carried on makeshift stretchers for hours or rely on sporadic, expensive private vehicle hires to reach the Shripur Health Center or beyond. Recognizing this, the health center’s in-charge, Mr. Mohan Datt Kalauni, initiated talks with Mr. Keshav Datt Kalauni, Chairman of the Jay Nagarjun Farmers Group. The farmers’ group, already a collective for agricultural development, saw this as an extension of their service to the community. The result was a pragmatic, incentive-based MoU that mobilizes local two-wheeler and four-wheeler owners as a quasi-ambulance network.
How the “Fuel-for-Service” Model Works
The agreement’s mechanics are beautifully simple and transparent, tailored to local realities:
-
Identification & Verification: The Health Center maintains and verifies data of emergency patients and the drivers who transport them. It is the sole authority to certify a case as an “emergency,” preventing misuse.
-
The Fuel Incentive: The farmers’ group commits to reimbursing drivers with fuel. The rates are fixed: 1 liter of petrol for a motorbike covering up to 30 km to transport a patient, and 1 liter of diesel for a four-wheeler covering up to 10 km.
-
Beyond the Ward: For cases referred outside Ward No. 3 or beyond the municipality, the support scales up. If the health center cannot treat a patient and refers them further, the farmers’ group will provide fuel—up to a maximum of 15 liters for long-distance referrals—ensuring patients reach higher facilities.
-
Accountability: Drivers must submit copies of their vehicle licenses and bill books to the group, ensuring only legitimate operators are part of the network. The health center provides a contact list of these drivers to community volunteers and representatives.
-
Timely Payment: All claims are settled by the farmers’ group within the first week of the following month, ensuring drivers are compensated promptly, sustaining their willingness to participate.

Impact: More Than Just Transportation
This MoU addresses multiple layers of the healthcare access problem in rural Nepal.
-
Immediate Response: It drastically reduces the “golden hour” gap in emergencies. A phone call can now mobilize a known, nearby driver, coordinated through the health post.
-
Economic Shield: For poor families, the sudden cost of transporting a patient could be catastrophic. This system removes that financial barrier, ensuring decisions are based on medical need, not pocket depth.
-
Community Ownership: The model fosters profound community ownership. The farmers’ group is not an outside NGO but a local entity investing in its own people’s welfare. The health post acts as the regulatory and medical anchor.
-
Sustainable Model: By using fuel as incentive—a tangible, needed commodity—rather than complex cash transactions for service, the system is easy to understand, administer, and trust. It leverages existing assets: private bikes and cars.
Challenges and the Road Ahead
The agreement is not without its challenges. It relies heavily on the integrity and availability of volunteer drivers and the health center’s diligent verification. The funding for the fuel comes from the farmers’ group, which may need to seek donations or allocate a portion of its collective funds sustainably. Monitoring referrals and preventing false claims will require continued strong coordination.
However, the very existence of this formal pact is a triumph. It demonstrates how local institutions can creatively collaborate within limited resources. It is a blueprint that other remote wards and municipalities across Nepal could adapt.
A Symbol of Self-Reliance
In an era where communities often look upward for government solutions, the Shivanath model is a powerful story of horizontal problem-solving. The signatories—Mohan Datt Kalauni of the Health Center and Keshav Datt Kalauni of the Farmers Group—have shown that the most resilient social infrastructure is often built by neighbors, for neighbors.
As this agreement is implemented, it promises more than just timely patient transport. It promises hope. It assures a mother in labor, a farmer with a fracture, or a child with high fever that their community has a plan to get them to care. In the demanding geography of Baitadi, this pact is a testament to the fact that when a health post and a farmers’ group come together, the distance to life-saving care can be measured not just in kilometers, but in the collective will to overcome them.
More News Click
This model stands as an inspiring example of local innovation, proving that sometimes, the most advanced healthcare logistics solution in a remote area is a signed piece of paper, a list of phone numbers, and a shared commitment to human life.